

































Robert F. Kennedy Jr., as the 26th Secretary of Health and Human Services, is right to force a reckoning on wireless-radiation policy. The public framework still in force allows 0.08 W/kg whole-body RF exposure and 1.6 W/kg peak spatial SAR over 1 gram of tissue for the general population. In 2021, the D.C. Circuit held that the FCC had not given a reasoned explanation for retaining its framework as to children, long-term exposure, pulsation or modulation, newer technological conditions since 1996 including the ubiquity of wireless devices and Wi‑Fi and the emergence of 5G, and environmental effects. That is not a settled safety regime. It is an unresolved regulatory failure.
Congress already gave HHS the job. Through the Radiation Control for Health and Safety Act of 1968, now codified in 21 U.S.C. §360ii, federal law says the Secretary shall establish and carry out an electronic product radiation control program designed to protect public health and safety from electronic product radiation, and shall plan, conduct, coordinate, and support research to minimize emissions and exposure. In other words, a serious HHS-led reset is not mission creep. It is exactly what the statute requires.
The thermal-only story has run out of road
The central weakness in current policy is that it still treats RF injury mainly as a heating problem. A 2022 analysis in Environmental Health argued that the FCC/ICNIRP framework still rests on assumptions carried forward from the 1990s and highlighted that the FDA nominated RF radiation to the National Toxicology Program because existing exposure guidelines were based on protection from acute thermal injury and might not be protective against non-thermal effects of chronic exposures. Once the governing system itself recognizes that acute-heat logic may be incomplete, pretending that compliance equals modern biological safety stops being serious science.
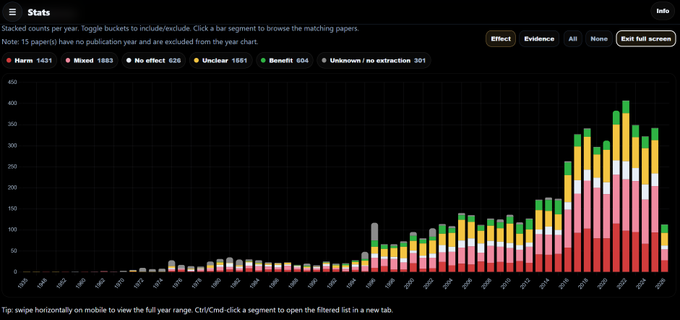
The strongest reason RFK is right is the animal cancer record. NTP says its two-year cellphone-radiation studies found clear evidence of malignant heart schwannomas in male rats, some evidence of malignant gliomas in male rats, and some evidence of adrenal tumors in male rats. The NTP technical report went further, describing clear evidence of carcinogenic activity in male rats for both GSM- and CDMA-modulated 900 MHz exposures based on malignant schwannomas of the heart, with malignant gliomas also related to exposure.
The raw tables are why this issue never died. In male rats exposed to GSM, malignant glioma rates were 0/90 in controls, then 3/90 at 1.5 W/kg, 3/90 at 3 W/kg, and 2/90 at 6 W/kg; glial-cell hyperplasia was 0, 2, 3, and 1. In male rats exposed to CDMA, malignant heart schwannomas rose from 0/90 in controls to 2/90, 3/90, and 6/90 across the three exposure levels. Those are not the markings of a biologically silent exposure. They are long-term tumor signals in the exact organs that have anchored concern in this field for years.
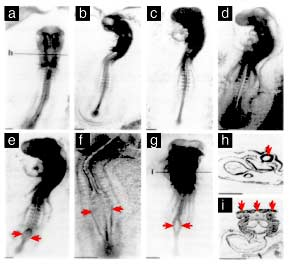
Ramazzini made the problem harder to dismiss, not easier. ICNIRP’s own synopsis of the Ramazzini study says Falcioni and colleagues exposed rats from gestation until natural death to 1.8 GHz GSM base-station radiation at whole-body SARs of 0.001, 0.03, and 0.1 W/kg for 19 hours a day, and reported a statistically significant increase in heart schwannomas in male rats at 0.1 W/kg. Two independent lifetime rat programs, using very different exposure regimes, converging on the same rare tumor class is exactly why this issue kept surviving every effort to wave it away.
By 2025, the formal evidence grade had moved upward. A major systematic review in Environment International evaluated 52 animal studies, including 20 chronic bioassays, and judged the certainty of evidence to be high for increased glioma and high for malignant heart schwannomas in male rats. IARC’s Advisory Group then recommended radiofrequency radiation for high-priority reevaluation because new human cancer and animal cancer evidence now warrant re-evaluation of the classification. That is not the language of a question that has been put to rest.
Fertility and child protection make delay indefensible
The case is not just cancer. In the WHO-initiated reproductive review track, the corrected analysis for pregnancy rate after male RF exposure changed from an odds ratio of 2.42 with moderate certainty to 1.91 with high certainty. The 2026 Environmental Health risk-assessment paper summarized the state of the literature bluntly: recent WHO-commissioned systematic reviews concluded with high certainty that RF-EMF increases cancer risk and reduces male fertility in experimental animals. Once fertility moves into that territory, the issue stops being a narrow academic dispute. It becomes a generational public-health issue.
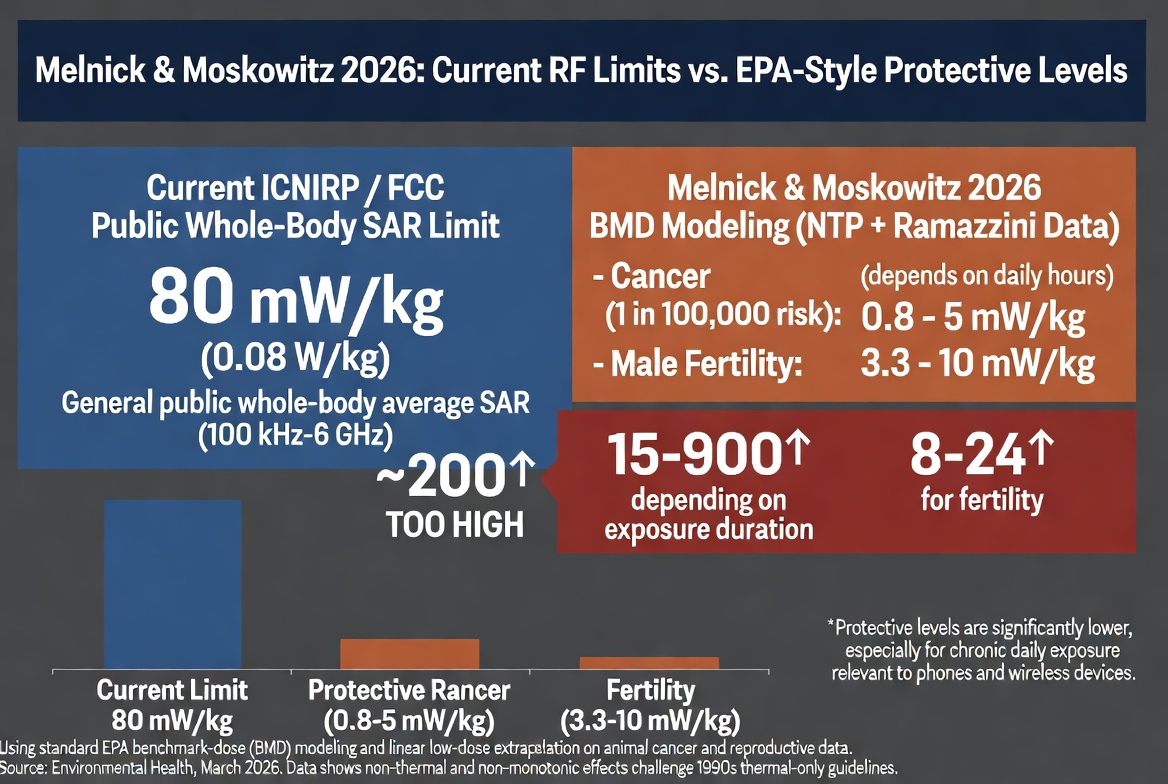
That 2026 paper is one of the strongest documents RFK can put on the table. Using benchmark-dose analysis for cancer and standard toxicological uncertainty methods for fertility, it estimated health-protective whole-body RF exposure values of about 0.8 to 5 mW/kg for a 1-in-100,000 cancer risk and 3.3 to 10 mW/kg for male-fertility protection. It then compared those values with the FCC/ICNIRP general-public whole-body limit of 80 mW/kg and concluded that current public limits are 15- to 900-fold higher than the cancer-protective estimates, depending on daily exposure duration, and 8- to 24-fold higher than levels protective of male reproductive health. That is not a small standards tweak. It is an indictment of the current ceiling.
Children make the failure even more obvious. A 2018 dosimetry paper reported that, compared with adult models, children experience two- to three-fold higher RF doses to localized areas of the brain when a phone is held at the ear, and to the eyes and frontal lobe when a phone is used for virtual reality. The authors said these findings raise serious questions about the current approach to certifying phones, particularly the use of the adult male SAM phantom. The D.C. Circuit echoed that concern, holding that the FCC’s explanation on children was arbitrary and capricious because the agency had not answered the real question: whether exposure allowed by the existing limits can harm children.
The newer Japan and Korea studies do not erase this record. The Japanese paper explicitly said it was not intended as a direct replication of NTP. The Korean paper said 70 males per group gave limited statistical power for detecting rare tumors, used only a single 4 W/kg CDMA condition, and selected that exposure level because 4 W/kg is the animal reference point behind current human limits. In the Korean tumor table, endocardial schwannomas appeared only in the RF-exposed group, 2/70 versus 0/70 in both control groups, though without statistical significance. Those studies narrow the discussion at one condition. They do not wipe out the broader multi-dose NTP and lifetime Ramazzini evidence base.
The non-thermal question is no longer hypothetical
FDA’s 2023 TheraBionic P1 approval matters here because it demolishes the lazy slogan that low-power RF cannot do anything biologically meaningful unless it heats tissue. FDA describes TheraBionic P1 as a handheld RF electromagnetic-field generator that emits specific amplitude-modulated frequencies which may stop cancer cells from dividing. FDA’s safety materials also warn against use with calcium-channel blockers and cite Cav3.2 T-type voltage-gated calcium channels and calcium influx in the referenced mechanism literature. Its importance for this debate is proof of principle: biologically meaningful RF interaction is real enough for FDA to regulate in a therapeutic device context. The blanket claim that non-thermal RF is inherently inert is no longer credible.
Federal action is indispensable because federal law blocks state and local governments from regulating the placement, construction, and modification of personal wireless facilities on the basis of the environmental effects of RF emissions when those facilities comply with FCC rules. If the national standard is outdated, the public is trapped under it. That is why RFK is right to press for an independent reassessment of FCC limits, a restart of serious federally supported RF-health research under 21 U.S.C. §360ii, child-specific compliance models, and immediate precautionary guidance where children and heavy users are most exposed. Even NTP says the public should reduce cellphone exposure by using phones less and putting more distance between the head and the device through speaker mode or a headset. Backing that agenda is not extremism. It is the evidence-based position.